

Why do wealthy Anglosphere countries have such poor mental health statistics? The Lovepost’s Capitalism and Mental Health series investigates this wealth-health paradox—and imagines doing things differently. Part 1 examines how neoliberal capitalism led to, and continues to have, devastating impacts on mental health, especially in high-income Anglosphere societies. Part 2 turns inward to highlight the internalised baggage of capitalism. How did unhealthy beliefs and values come to feel so normal? Part 3 investigates modern psychiatry’s treatments, focusing on how external pressures shaped a framework exploited by pharmaceutical companies, leading to harmful, pharmaceutical-centric approaches that influence mental health policies and public perceptions to this day.
If you accept that you have an abnormality in your brain, and there's this drug that can put it right, of course, you would take it, wouldn't you?
—Dr Joanna Moncrieff, psychiatrist and professor, in conversation with The Lovepost.
Mental health care in high-income countries has undergone rapid transformations since the late 1970s. The advent of new diagnostic manuals, alongside targeted psychiatric drugs, neuroscience technologies, psychotherapies such as cognitive behavioural therapy (CBT), and a massive increase in funding and care investment should have eased the burden of mental illness for society and the individuals suffering from it. Yet across high-income societies, the much-celebrated breakthroughs have coincided with exponential growth in people with mental health disorders.
The statistics are concerning. Even when mitigating population growth, more people are on benefits for anxiety, depression and substance abuse than ever before. According to Johns Hopkins Medicine, 26 percent of Americans aged over 18 will suffer from a diagnosable mental health condition in a given year. The rate of one in every four people is similar in the United Kingdom, with New Zealand, Canada and Australia tailing very close behind. In all countries, prevalence is trending upward.
Diagnosis rates have coincided with a staggering increase in the number of people consuming psychiatric drugs. In 2021, the global market for these drugs neared 40 billion USD and is projected to rise to almost 59 billion USD by 2031, with an expected increase in mental health disorders igniting growth in the market. The market for Major Depressive Disorder (also known as clinical depression) is predicted to “register stunning growth” as case numbers grow between now and early next decade.
Even before COVID-19 blasted prescriptions sky high, antidepressant drug use alone more than tripled in the United Kingdom over the last 23 years from 18.4 million in 1998 to 83 million in 2021. Similarly, rates in the United States have increased by 65 percent since the 2000s, with one in eight Americans on antidepressants.
Do these statistics show that more people are now receiving treatment because of better access to mental health and addiction services? The New Zealand Ministry of Health thinks so, describing the 20 percent growth in prescriptions for antidepressants between 2010 and 2022 as positive; the rise signals we may finally be free from the pernicious social legacy of stigmatisation and reticence about our mental health issues.
In contrast, an increasing number of psychiatrists, psychologists, academics and researchers are collectively voicing concern over these statistics. These theorists, who we spoke with for this story, argue that in the 1980s, psychiatry adopted a new understanding of distress, which radically revised how human emotional reactions are understood and how best to treat them.
Overreach: the medicalised model of mental disorders
[Mental illness] is a medical condition, just like heart disease or diabetes. And mental health conditions are treatable.
—American Psychiatric Association
The American Psychiatric Association (APA) developed the Diagnostic and Statistical Manual of Mental Disorders (DSM) to standardise the diagnosis of mental health conditions and create a common language and criteria for mental health professionals. The first editions, DSM-I (1952) and DSM-II (1968), were an attempt to make sense of mental health disorders in a more organised way that would serve as a reference point for clinicians. Both were very much products of their time, with many conditions understood to arise via suppressed unconscious forces (think Sigmund Freud). Despite the DSM's best intentions, these abstract hypothesised forces remained extremely difficult to examine empirically or systematically.
The third edition, DSM-III, published in 1980, was a significant and wide-reaching break from earlier versions and remains the conceptual basis of all subsequent versions of the DSM. The manual was the platform for an international paradigm shift in clinical and cultural understandings of human distress. It’s important to note that while the World Health Organization has its own globally influential categorical system—it also adopted the DSM III’s focus on observable symptoms for the International Classification of Diseases (ICD), from the 10th edition onwards.
Both those who think current mental health statistics in the Anglosphere reflect the actual prevalence of disorders and those who think the definitions partly manufactured the rates of illness explain their views with reference to this milestone.
Robert Whitaker is a former director of publications at Harvard Medical School, Pulitzer Prize finalist, and founder and director of the prominent Mad in America: Science, Psychiatry and Social Justice webzine (named after his 2003 book). He thinks the DSM-III is the basis of overdiagnosis and the resultant over-medicalisation of vulnerable people.
Whitaker’s perspective is informed by his research into American psychiatry’s historical attempts to achieve medical legitimacy. He explains that issues and scandals, particularly those in the early 1960s, undermined psychiatry’s professional legitimacy. One problem was reliability issues with listed disorders in earlier versions of the DSM.
“Studies showed the DSM and DSM-II disorders weren't validated disorders; they weren't reliable within medicine,” Whitaker says. “A diagnostic manual to be worthwhile is supposed to have two qualities.
“It's supposed to be reliable. I go to you or another doctor and get the same diagnosis. And it is supposed to be valid; in other words, diagnosis is supposed to be, for some disease, with some criteria for saying this is different from another disease.”
Whitaker observes that questions about the reliability of the early DSMs coincided with the infamous ‘Thud’ social experiment. Psychologist David Rosenhan and seven other ‘pretenders’ presented to psychiatrists at Harvard State University, claiming to hear voices and were committed and medicated. The experiment proposed that the psychiatrists and other mental health staff could not differentiate between the sane—those acting—and the clinically insane.
Within universities, an anti-psychiatry movement also gained prominence and popularised public suspicion in line with the anti-establishment tones of the 1960s. These anti-psychiatry advocates painted psychiatry as an agent of social control—an extension of the prison system—for people who did not conform to society’s expectations and norms. This sentiment was further promoted by cultural works such as Ken Kesey’s One Flew Over the Cuckoo's Nest, which satirised and increased distrust in psychiatric authorities.
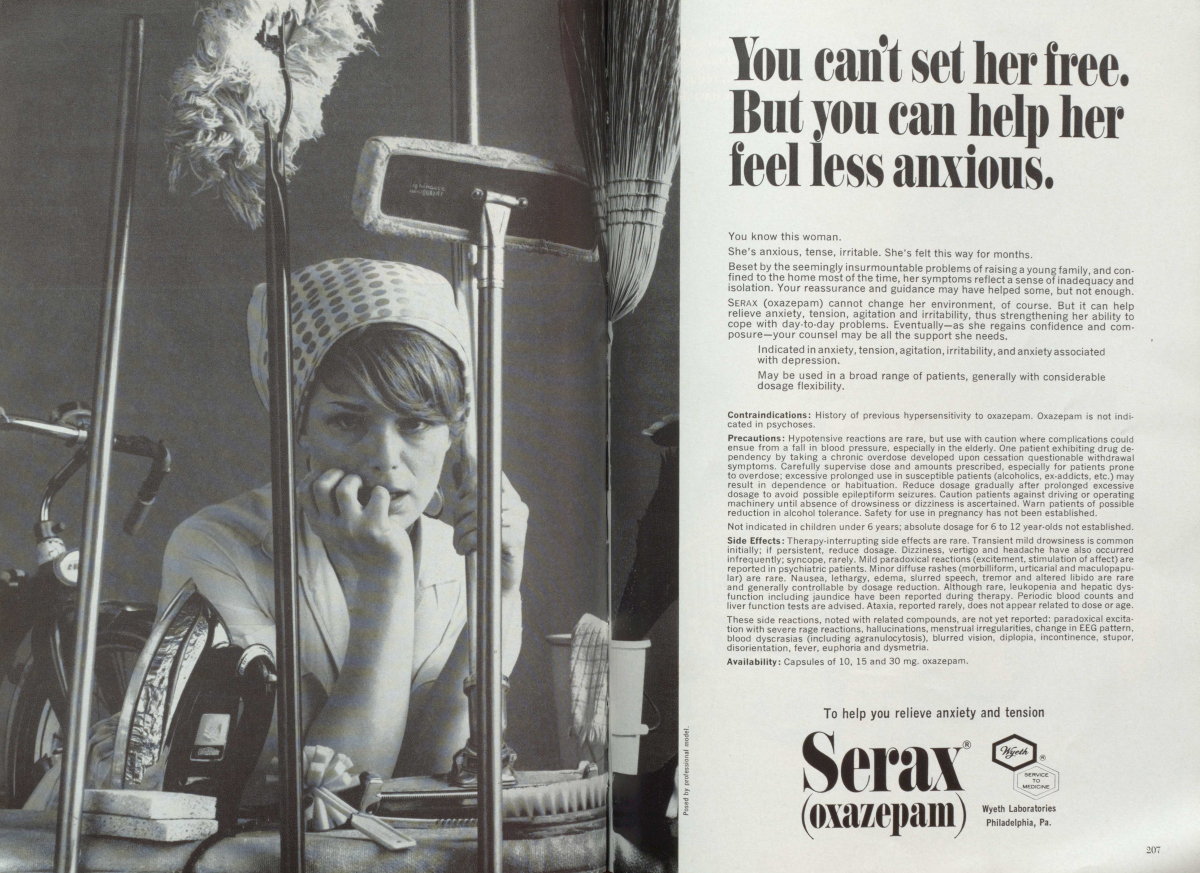
Jerome C. Wakefield is a New York University (NYU) professor and co-author of The Loss of Sadness: How Psychiatry Transformed Normal Sorrow into Depressive Disorder. Like Whitaker, he recalls the many scandals that undermined American psychiatry at the time. He remarks that the overprescription of addictive tranquillisers, such as Valium (Diazepam), in the 1960s and 1970s played a major part in psychiatry’s ill repute: “There are amazing studies from the ‘60s and ‘70s that showed that, no matter what you went to a physician for, whatever physical problems, psychological problems, anything... 20 or 25 percent of all visits resulted, whatever else they gave you for your problem, they gave you a Valium prescription as well… to keep you calm about your problem.”
Not incidentally, women were major consumers of these drugs, dubbed 'mother's little helper' by The Rolling Stones.
The American overprescription scandal provoked government intervention. Resultant legislation meant that the federal Food and Drug Association (FDA) would only approve drugs that acted on established and validated medical conditions. As psychiatrists tended to refer to their own clinical reference points and not those set in medical science, their treatment options were severely limited. Adding to the mix of challenges, health insurers increasingly demanded that psychiatry show that its treatments were targeted and effective before funding treatment.
The release of the DSM-III represented psychiatry's reply to its critics and embodied the field’s desire to make psychiatry more medical and scientific and, thus, it was assumed more reliable. Representing a considerable break from previous editions, the DSM-III left the ‘how and why’ of disorders to competing theories. Clinical diagnoses were freed from the ambiguity and complexity of a search for underlying causes as debated in the many different strands of psychology, psychiatry and social sciences.
The DSM-III's new framework neatly grouped disorders by observable and self-reported symptoms. It established and provided symptom lists for the now widespread afflictions of Major Depressive Disorder (MDD), Bipolar Disorder, Post Traumatic Stress Disorder (PTSD) and the subsequently rebranded Attention Deficit Hyperactivity Disorder (ADHD).
It’s important to reflect here on the transformative impact of the disorder classifications that the DSM-III introduced: the classification of depressive symptoms offers a compelling snapshot. The DSM-III comprehensively redefined the classification of depressive disorders, merging previously distinct forms of depressive experiences into a single category. It combined the extreme form of psychotic melancholia—characterised by a vegetative state, delusional thinking, and hallucinations—with a revised conception of ‘neurotic depression.’ Before the DSM-III, ‘neurotic depression’ was believed to be a feature of broader conditions, like anxiety, and not a depressive category in its own right. Including milder states within the parameters of disorders is a site of ongoing debate and controversy.
Sick societies: loosen the criteria, and more people get sick
Dr James Davies is a British National Health Service (NHS) psychotherapist, Associate Professor of Medical Anthropology and Psychology at the University of Roehampton and author of the 2021 book Sedated: How Modern Capitalism Created Our Mental Health Crisis. He notes that since the introduction of the DSM-III, the number of listed mental disorders has risen from 100 in the 1970s to nearly 300 presently.
According to Davies, “Not only did the number of mental disorders believed to exist expand, but what the manual did from the 1980s onwards was progressively lowering the bar on what constitutes having one of these disorders, in effect making it far easier for any of us to be classed as mentally ill.
“By expanding the definition of mental illness to encompass more and more domains of human experience, more and more of us would identify as mentally disordered, ill or unwell.”
Drawing on his research into medical anthropology, Davies also thinks the universalising assumptions of the DSM are increasingly problematic. He highlights the DSM-III was not a product of the then-current research literature or systemic study; rather, it emerged from the decisions of "a small culturally homogenous subset of mental health professionals in positions of influence." This determination was made through the cultural activity of a vote-based consensus, a process that Davies deems ethically and scientifically problematic.
It’s problematic to him because the DSM identifies and distinguishes symptoms within the socioeconomic norms of American and other high-income societies in the 1980s. This inevitably privileges a Western understanding of illness and conceptions of a healthy person as perceived during that specific and unique period of time. As societies have become more cognisant of cultural diversity and the structural impacts of race and colonisation, psychology and psychiatry's universalising language (of fixing abnormal people) and practices are increasingly under scrutiny and contested.
Several studies highlight that some DSM disorder classifications may not universally apply, potentially contributing to stigmatising culture-bound expressions of distress that deviate from clinical expectations. The impact of cultural influences on emotional expressions is significant, as specific symptoms can be rational responses within distinct cultural norms or contexts.
Furthermore, in some cultures, distress symptoms may manifest in the body, such as physical pain, diverging from the psychological emphasis observed in Western contexts. While people worldwide may experience similar subjective pain, the triggers, interpretations, symptoms and social labels for their suffering can vary significantly. This diversity is also evident in communal approaches to mental illness, more prevalent in non-Western contexts, which contrast with the individualistic focus of the DSM.

False positives: is grief a mental disorder?
In his office at New York University, Wakefield researches DSM 'false positives,' which occur when the diagnostic criteria capture distressing emotional or cognitive experiences that echo but are not bonafide disorders. Wakefield thinks false positives occur because "there is virtually no psychiatric symptom that doesn't also occur under normal conditions at some point."
Acknowledging this, the DSM-III introduced exclusion clauses to protect reasonable emotional responses to stressful life challenges, such as losing a job or divorce, from diagnosis and medicalisation. Problematically, some of these have been removed. A case in point is the 2013 release of the fifth version of the DSM, which controversially removed the ‘bereavement exclusion’ from the diagnosis of Major Depressive Disorder (MDD).
The exclusion told clinicians to avoid diagnosis if the recent loss of a loved one was a catalyst for a person’s symptoms of depression. The APA reasoned that this would help a group of individuals experiencing prolonged and debilitating grief who were suffering from feelings of worthlessness or thoughts of ending life. They justified the removal via empirical research, which found that loss can precipitate MDD and, if extreme and enduring, is essentially indistinguishable from MDD symptoms.
Wakefield believes that removing exclusions fuels overdiagnosis and delegitimises people’s lived experiences. By conflating a mental disorder with the inevitable and natural human process of grieving, individuals in mourning are being labelled as abnormal and told by clinicians they need medication to ease their emotions. He doubts that psychiatric drugs are really the crucial support many grieving people need.
Five years later, the writers of the most recent manual responded to the controversy. Instead of acknowledging that grief sets its own calendar, they created the DSM’s newest disorder: Prolonged Grief Disorder, which, while still diagnosing and medicalising grief, cedes to critics such as Wakefield that it's not a form of MDD and sets six months for children and one year for adults as its boundary points for onset.
Wakefield thinks diagnostic overreach is also caused because the DSM-III cannot distinguish between dysfunctions of evolved biological traits and those causing the person harm in the societies in which they live. Imagine, for example, someone who is naturally very active and alert—these are traits that helped our ancestors survive. But if this person lives in a society where everyone is supposed to be calm and quiet, the DSM might say they have a mental disorder.
Like Davies, Wakefield worries that without a clear boundary, DSM categories can encourage the pathologisation of people for culturally divergent behaviours, attributes and thought patterns as "one of the basic tools of social regulation is to portray what society wants from people as natural, as biologically designed."
Wakefield continues that because psychiatry remains uncertain about the fundamental causes of disorders, “intuitions about what's socially desirable and socially adaptive [can] get confused with intuitions about what's normal and disordered.”
Wakefield means that societies often try to convince people that their expectations and rules are not simply societal constructs but are how human beings are naturally supposed to be. This can be a way to encourage conformity and discourage behaviours or traits that deviate from what dominant forces in society consider acceptable.
Dr Bruce Levine, a Cincinnati-based clinical psychologist, author and social critic, has written extensively on the concerns Wakefield and Davies raise. His writings emphasise the damage that blurring social norms with mental disorders can do to groups of people. He thinks homosexuality—reframed in the DSM-III to the controversial Ego-Dystonic Sexual Orientation Disorder—is an explicit example of the medicalisation of behaviours that do not align with dominant cultural norms and values.“When young gay individuals were pathologized by psychiatry . . . some died by suicide because they did not want to live with the belief that they were defective,” Levine says. “Still, others became politically and artistically radicalized—not only distrusting mental health authorities but other societal authorities as well.”
Levine notes that the removal of the disorder in the 1987 revision of the DSM-III was due to changing social values and laws, which psychiatry had to assimilate—not any evidence-based advances or insights into diagnostic categorisation.
Wakefield and Davies think the need to differentiate between actual disorder and non-pathological human suffering, eccentricity or cultural variation is of social concern in a pluralistic society. For example, Wakefield states that rather than diagnosing a hyperactive kid for failing to adapt to the sedentary expectation of modern society, it would be more humane to change the social situation promoting distress or problematic behaviour: the school environment should be changed to be more inclusive of children with different temperaments.
Collectively, Wakefield, Davies and Levine believe that when psychiatry treats people who are not really mentally disordered, it is no longer primarily a medical field treating legitimate clinical conditions—it’s more like a peacekeeping force for the failure of other more appropriate non-medical support systems. Robert Whitaker, from Mad in America, also believes over-diagnosis limits our humanity.
“Think of Shakespeare,” Whitaker says. “They're all like, jealous, envious and crazy. They have feelings of violence, and that's the greatest theatre ever. We identify with these people, right? Every one [of those characters] would be diagnosed. There is not a single Shakespeare character who would not be diagnosed in the DSM.”
The DSM indirectly links mental disorders to brain diseases
The clarity of the DSM-III framework enabled it to be quickly adopted in clinical settings. Psychiatrists and physicians began to diagnose people using the DSM-III’s short generic checklists of symptoms—the more the patient exhibited, the more likely they were to have a mental health condition. Wakefield thinks that despite its enduring problems, the DSM-III's symptom-based criteria was a significant step forward in pursuing standardisation across psychiatry and has led to greater efficiencies in diagnosis and reporting.
However, one of these enduring problems is that the DSM-III sought to reinforce the medical legitimacy of psychiatry—particularly its supremacy over psychology and the social sciences—by implicitly associating many mental disorders with physical disorders. Adopting medical disease classification systems and rejecting psychological theories and terms, such as 'neurosis', marked the new prominence of biological and neurological explanations in psychiatry.
Even if the DSM-III avoided overt conclusions about a disorder's causation—its crisp classifications indirectly promoted the idea that people suffered from mental disorders in the same way that they have diseases like diabetes.
As the 1980s progressed, new mathematical and neurological understandings of brain behaviour gained prominence and prestige. As a result, the belief that mental disorders are primarily products of biological abnormalities in the brain became more explicit and assumed. This model suited targeted and controlled research in a way broad understandings involving psychological, social and cultural differences could not. Radically reductive and isolated research was favoured—as only this could produce reliable, scientifically informed empirical evidence. Anything too complex or messy was too difficult to test empirically and was avoided. Through this research, particularly in neuroscience, disorders become associated with problems of specific physiologies, especially brain processing dysfunctions. Importantly, this scientific research and its promotion strengthened the professional validity of psychiatry as an evidence-based professional body.
Wakefield thinks the turn towards biological understanding was not problematic conceptually; it’s a legitimate base for researchers to analyse mental disorders as it is self-evident that all evolved beings experience variations due to biological variations. Even if the exact causal genetic markers and brain processes remain hypothetical, intuitively meaningful or only ever partially known, it has and will continue to provide profound insights into understanding mental health disorders.
Whitaker is less positive about the shift. He interjects that the biological and brain conceptualisation of mental health has become much more than a research perspective.
Whitaker says that while physiological model hypotheses are sometimes compelling, most DSM disorders have no biological markers and remain hypotheses and constructs. It’s alarming to Whitaker that understanding of mental illness became so comprehensively tied to specific brain diseases in the absence of conclusive research: “There were and are still no physical tests for mental disorders, no brain scans,” he says. The research that has been done finds the DSM categories map poorly with dysfunctions of brain circuits or neurochemical pathways.
Dr Joanna Moncrieff, a psychiatrist and a professor of critical and social psychiatry at University College London, shares Whitaker’s perspective. She argues that attaching unsubstantiated claims of brain disease to DSM diagnoses creates a harmful misconception of mental illness, with far-reaching consequences for both society's understanding and the lives of those affected.
She tells The Lovepost that because we still do not understand what causes many proposed mental illnesses, psychiatric diagnoses are not the same as medical diagnoses. They are instead and remain a generic classification system for human problems.
“In medicine . . . most diagnoses tell you something about the nature of the problem.” Moncrieff says. “So with liver cancer, you have a tumour in your liver. In chronic obstructive airway disease, you have a pathological process going on in your lungs.
"[But] psychiatric diagnoses do not tell you the cause of the problem. They are simply labels for various forms of behaviour and reported feelings and experiences that people report.
“People absolutely don't get that and think that a diagnosis is telling them something they didn't know about themselves. The only thing it might tell people is that your problems are a little bit like some other people's problems.”
Moncrieff believes that patients and their families assume health professionals can make health-enhancing decisions based on biomedical evidence through classification. However, the assumption is incorrect, stemming from sustained publicly sanctioned misinformation that needs dismantling to provide effective and humane care for distressed people.

Big Pharma: marketing misinformation and the commodification of suffering
The DSM-III's universalising and loosened symptom-directed approach and the professional favouring of brain research explanations have contributed to the prevalence of reported mental distress in the Anglosphere. But that’s only part of the story.
Alarmingly, the dramatic upsurge in diagnosed mental disorders from the 1980s can be attributed to the influence of pharmaceutical corporations—who have shaped, oversimplified and distorted mental health understandings through their pervasive marketing efforts.
Whitaker says that the pharmaceutical industry conveyed this message as a simple action statement: “Pharma needed to come up with a new narrative, and the new narrative was, 'you have a chemical imbalance, you have a brain disease, and we have the treatment for it’.” The mantra became an extremely effective public marketing campaign taken on by government and health bodies under the guise of public education. The narrative provided health centres with more straightforward and cost-effective treatment choices. It also sold people a path to relief from often debilitating states of distress.
The DSM’s symptom-based classifications served as a stimulant, paving the way for pharmaceutical companies to cultivate a flourishing market for products addressing these new broad categories of mental distress.
“I don't believe that psychiatrists purposely create criteria for their pharma friends,” Wakefield says. “I think they're sincerely creating criteria they think will help people, but [some of these] are inaccurate.
“What happens is the big pharma companies do what they're paid to do. They say, 'Oh, look, the depression criteria have nine criteria, and these five are pretty weak. If we emphasise those, we can hit 25 percent of the whole population as . . . potentially disordered and get them to come in and get help’.”
Treatment for less acute depression and anxiety become a major target for industry growth. With the DSM-III unification of severe and mild forms and a clear list of criteria, drug companies could highlight the effect of a drug on treating distressing symptoms for a large group of people. Similarly pivotal, aspects of the medications with negative effects that did not correspond to symptom relief could be separated as unintended ‘side effects'. The question became whether the side effect outweighed the proposed symptom relief—a whole new way of presenting and reporting about psychiatric drugs.
With the new regulatory requirements in mind, and with the DSM as a blueprint, Big Pharma developed and unleashed a whole new generation of drugs like Serotonin Selective Reuptake Inhibitors (SSRIs)—think Prozac—to target the symptoms and deep causes of depression. Pharmaceutical companies relentlessly pushed chemical imbalance theories to explain how their antidepressants correct abnormal brain functions. In their advertisements, they claimed that mental health problems, like depression, were due to imbalances in neurotransmitters and that their medications could fix this by returning serotonin to their normal levels. The new Big Pharma reading compared mental conditions to physical conditions like diabetes and antidepressants to insulin.It was a powerful and convincing message. In the haze of the marketing frenzy, there was no need for truth to get in the way of a good story. A 2005 study into the disconnect between pharma-mediated public-facing information about SSRIs and the evidence base led the authors to conclude that the “incongruence between the scientific literature and the claims made in FDA-regulated SSRI advertisements is remarkable and possibly unparalleled.”
The Big Pharma-fest: to build a market, influence the professionals
While most high-income countries (excluding the United States and New Zealand) forbid direct-to-consumer marketing of psychiatric drugs, pharmaceutical companies found an effective avenue by sponsoring and advertising their drugs directly to psychiatrists, clinicians and health bodies. After all, it is them whose expertise patients would ultimately defer.
Whitaker and Davies have written extensively about the profound impact of pharmaceutical companies, detailing sustained, exorbitantly funded, and remarkably successful marketing campaigns. Strategically, the industry aimed these efforts at influencing mental health authorities, psychiatric associations, and clinicians to endorse and prescribe their pharmaceutical products.
The industry heavily invested in research into mental disorders and training in mental health care. In 2012, Big Pharma sponsored nearly every major scientific journal and meeting in psychiatry. Similarly, Pfizer sponsored DSM researchers to develop symptom-based checklists, such as the PHQ-9 depression checklist, and then distributed them.
Davies also revealed that pharmaceutical firms purchased vast numbers of the DSM-5, propelling it to the top of Amazon’s bestseller book list—illustrating the enormous scope of their impact and the DSM's pivotal role in their market approach. Subsequently, pharmaceutical sales representatives distributed these copies at no cost to general practitioners and mental health centres across the United States.
Drug companies also sponsored networking conferences and rewarded the psychiatrists in attendance. Moncrieff describes some pharma-led education events as more like a holiday park or trade fair than a serious medical meeting. For example, 2001’s pharma-funded 7th World Congress of Biological Psychiatry included an artificial garden, a running stream, a giant rotating tower, and fortune-tellers. Many attendees had their international flights, accommodation and food paid for; they also received generous entertainment allowances. Moncrieff insists such lavish proceedings and benefits were once common practice. And they may well have been effective and not just perks of the job: physicians, including psychiatrists, are not immune to psychological marketing tricks, and studies show attending such events is linked to higher prescription rates.
The pharmaceutical industry manifestly believes paying psychiatrists and mental health clinicians is good for business. They persist despite policies and laws introduced to tackle the not-so-hidden scourge of conflicts of interest. In 2010, the Federal Physician Payments Sunshine Act passed, forcing United States-based drug manufacturers to track and report payments to physicians and teaching hospitals. In parallel, the APA revised its policy and required experts to disclose financial ties for work on the DSM-5.
Despite these changes, direct payments to United States psychiatrists totalled 340 million USD between 2014 and 2020. APA policy changes also had little effect; 57 percent of advisors to the DSM-IV had financial ties to pharmaceutical companies, but by the fifth DSM, that number had risen to 70 percent. These statistics caused Whitaker to retort: “They are not even trying to hide it anymore!”
The most problematic issue is pharmaceutical companies' role in developing the evidence base for the drugs they sell. It is this evidence base that clinicians rely on to justify drug prescriptions to patients. Authorities, such as the FDA, various health bodies and insurance companies, make decisions based on that body of evidence.
Pharmaceutical influence clouds the evidence base. An analysis of published studies on depression and antidepressants found that drug manufacturer employees were 22 times more likely to report industry-favourable drug outcomes than those who weren't. The effect of this bias becomes clear given that pharmaceutical company employees produced 30 percent of the studies. At the same time, another 79 percent of authors that received sponsorship were former employees or had declared conflicts of interest, leaving a minuscule three percent of the analyses without potential conflict of interest.
Davies tells The Lovepost that one infamous case of pharmaceutical evidence tampering was AstraZeneca's publishing of cherry-picked findings supporting their new drug Seroquel (Quetiapine), even when the studies they commissioned proved that the drug ‘was less effective’ than drugs already on the market. A leaked AstraZeneca email clarified that a selective butchering and suppression of contrary findings occurred in the final published study.
Whitaker provides another example. In 2010, AstraZeneca paid 520 million USD to settle a US Government lawsuit filed in response to the illegal marketing of Seroquel as a treatment of psychiatric conditions that the FDA had not approved. The case highlighted that the company targeted and financially incentivised non-specialist physicians who treat older people, children, adolescents, prisoners and people in long-term care. Given that the global revenue AstraZeneca earned from Seroquel was 4.9 Billion USD in just 2009 the slap on the wrist was unlikely to be much of a deterrent. Davies and Whitaker assert that such occurrences are not unique and not limited to AstraZeneca.
Publication bias—where beneficial studies are published and promoted, and pharmaceutical companies suppress negative clinical trials—has distorted the evidence base profoundly. For example, A 2014 meta-analysis of 70 clinical antidepressant trials involving over 18,000 people found widespread bias, unsubstantiated conclusions and recurrent study design flaws. The review found that crucial negative findings were either withheld or suppressed.
Some trial studies reframed suicide attempts as “worsening depression.” The report led a writer from Scientific American to state that “important data about the safety of these drugs—especially their risks for children and adolescents—has been withheld from the medical community and the public.”
For reasons also unrelated to people’s best interests, Big Pharma campaigns, sponsorship, and evidence-based tampering have limited lifespans. The patents for many drugs introduced and sold as chemical cures in the 1980s and 1990s have expired. With generic and much cheaper versions of the drugs available, Pfizer, Eli Lilly & Company, and AstraZeneca no longer make the windfall profits they earned while controlling them exclusively. Nowadays, they have less vested interest in influencing regulating policy and the experimental base supporting the drugs.
In this new environment, it becomes possible to separate pharmaceutical fact from fiction without the cloud created by Big Pharma’s influence. Unencumbered by the pursuit of staggering profits, what has happened to the heavily promoted pharma-driven disease model claims that imbalances in serotonin caused depression.
Depression: moving beyond chemical imbalances and antidepressants
A cascade of occurrences, including loosened diagnostic criteria, a shift towards biological analysis, new regulatory requirements, and pharmaceutical company opportunism and influence, established a pervasive belief that depression is a product of a chemical imbalance of neurotransmitters, particularly serotonin, and that antidepressants work to correct this imbalance.
In 2022, Moncrieff, a psychiatrist and a professor of critical and social psychiatry at University College London, and colleagues published their review of reviews on the serotonin theory of depression in the journal Molecular Psychiatry. The study analysed all published scientific evidence on the hypothesis. It concluded that “there is no consistent evidence of . . . an association between serotonin and depression and no support for the hypothesis that depression is caused by lowered serotonin activity or concentrations.”
Moncrieff’s review caused a media and public sensation. According to the research-metric site Altmetric.com, it is in the top five percent of articles—out of the 22 million research papers they have tracked—for the attention it generated. She was interviewed by dour radio news presenters, appeared on garishly lit TV breakfast shows and was featured in newspapers across the political spectrum. For many, the study was captivating because the chemical imbalance theory of depression had the aura of a long-accepted scientific fact; it's the reason many people consent to antidepressant treatment. According to The Guardian, thanks to Moncrieff, the theory is now well and truly dead.
The review ruffled the feathers of many psychiatrists and scientists. Some argued the review was a bit of a false flag as psychiatrists acknowledge the inadequacy of the association, and researchers have long abandoned simple serotonin imbalance hypotheses to explain depression. While conceding it's still unclear the effects of antidepressants on the brain, Professor of Psychiatry Zoltan Rihmer and colleagues note that “it has long been known that depression is a heterogeneous disorder not only genetically, clinically and biologically but also from a pharmacotherapeutic perspective.”
Moncrieff rebuffs that the theoretical uncertainty about the biological and pharmaceutical basis warrants serious reflection in public health discussions because of its implication for prioritised treatment choices. She notes that health bodies have long favoured the efficiency and shorter contact time involved in drug-based treatments because they are more cost-effective than other therapeutic models. Highlighting the unfounded dominance of drug-based mental health care calls into question the validity of this model of care with profound medical, social and policy implications.
She argues that if antidepressants are not scientifically established as targeted brain correctives, then alternative—and for Moncrieff, more plausible—explanations need to be considered. They might operate similarly to how earlier psychiatric sedatives were presumed to, and how drugs of abuse still do, by gradually dulling emotions over time, resulting in fewer highs and lows. “If these medications are more like alcohol, that’s a whole different kettle of fish,” Moncrieff said in an article for Psychiatry Online.
Moncrieff thinks the review underlies the profound disconnect between science, psychiatry and what is communicated to and understood by the public. Studies highlight this disconnect, showing that upward of 80 percent of people still believe the pharma-driven narrative about the causal role of serotonin imbalances in depression and that SSRI antidepressants work by correcting this imbalance.
A quick scan of websites, like the Royal Australian and New Zealand College of Psychiatrists, highlights the continued communication of the chemical imbalance narrative. Correspondingly, a 2020 study examined public-facing information about the benefits and risks of antidepressants in treating depression. The researchers examined the highest-ranking Google health-related websites in ten high-income countries, including websites run by government advocacy groups and healthcare providers. They determined none of the websites met established medical standards for informed consent or scientific evidence. Many distilled simplistic explanations about the biological foundations of depression. The researchers concluded that the “information was generally inaccurate and unhelpful and had the potential to lead to inappropriate use and overuse of antidepressants.”
Discussing Moncrieff's review with The Lovepost, Whitaker defines the vital issue: the APA’s internal training manual contradicted 'chemical imbalance' theories, yet their public website continued promoting the link for years. Problematically, the APA did not prohibit pharmaceutical companies from utilising the theory to market their drugs. Whitaker contends that this raises serious questions about the APA’s responsibility to inform the public, especially people prescribed the drugs.
“It raises a whole host of issues with informed consent,” he states. “It raises the questions—why did the public believe otherwise, and what is the responsibility of a guild to communicate and be honest about what they know?”
Moncrieff agrees, asserting that health bodies and professionals bear a duty of care to debunk industry-serving myths. They must communicate uncertainty about brain chemistry interactions and acknowledge that some drug-induced interactions, particularly with long-term use, may extend beyond short-term side effects and pose potential harm. People offered antidepressants need to be aware that the evidence supporting the benefits of drugs in treating depression remains inconclusive, with limited efficacy, especially for milder forms. This information allows them to make informed decisions about drugs that directly affect and alter their thinking and emotional states.
The transparency Moncrieff advocates for is crucial for distressed people seeking help in medical fields for their problems. The persistent spread of false explanatory narratives encourages overreliance on pharmaceuticals and fosters patient passivity. The amalgamation of diagnosis and drug-based treatment significantly shapes how people perceive themselves, their problems and their potential for improvement.
“One of the things that worries me most about the whole narrative . . . is that if you are told that you have an abnormality in your brain that needs a drug to put it right, that is a huge thing to be told, isn't it?” Moncreiff says.
“That's a really serious thing to say to someone. And I think that people do internalise the idea that there is something defective about them. Something permanently wrong with their biology that they themselves, as a person . . . have no power to change. And that, of course, is really deeply disempowering.”
Whitaker adds that debunking the lingering pharma narrative is crucial to our social wellbeing: “We started seeing our kids and ourselves through this narrow thing and seeing ourselves as abnormal, chronically ill [and] pathologised. Well, that's like a self-fulfilling prophecy.“ If you're going to start having a philosophy of being that tells you to be alert all the time and if you have these uncomfortable feelings, something's wrong with you. You go to a doctor, and the doctor prescribes you a drug. What do you think's going to happen when you encourage a whole society to be worried about whether they're normal all the time?”
Moncrieff, Whitaker, Wakefield and Davies emphasise that their mission isn't a straightforward campaign to prohibit psychiatric drugs. Wakefield asserts that psychiatric drugs can and do help people who live with substantial disabilities. Moncrieff concurs, acknowledging that some individuals may undergo severe distress even in the most utopian societies. In such cases, drugs, with sound research into their risks, and accompanied by other social models of care, can offer assistance.
The common thread among all is a critique of the widespread use of unverified drug-based treatments in both mental health and primary care settings. They worry that healthcare practitioners, influenced by funding choices, may diagnose and prescribe drugs too readily, potentially causing more harm than good to individuals experiencing natural variations in cognitive differences and acute emotional responses.
They think that medicalising environmentally induced distress not only muddles an individual’s understanding of their suffering but also restricts access to a diverse range of care options, many of which are not medical, that could offer sustainable benefits to those in distress, their families and society.
“Last year in the NHS, about 8 million adults were prescribed an antidepressant compared to only one and a half million prescribed psychological therapy,” Davies states.
“This huge imbalance in provision doesn’t exist because people are going to the doctor and asking for drugs—in fact, the research says the opposite: people who go to a primary care facility because they are struggling invariably would prefer a social or psychological intervention, but that’s not what they are getting. This imbalance exists because this is the intervention we have privileged over a long period.”
The overprescription of pharmaceuticals to combat depressive symptoms, likely obscures the role of societal and economic forces, leading to an ineffective and potentially hazardous short-term solution that does not address the underlying systemic issues. This is the critical point of Davies's 2021 book, Sedated: How Modern Capitalism Created Our Mental Health Crisis, which outlines how market-influenced mental health systems have reframed natural human reactions to difficult circumstances so that we look to shortcomings in ourselves rather than the circumstances that compound our distress.
Davies explains that as a result, “we cease to understand that suffering is often a protest against these circumstances—a call for change, social change, rather than self-change. By being misled about what we need to do to overcome our distress, we are far less likely to overcome it.”
Towards systemic change: putting the social back in mental health care
It's clear that relying too heavily on broad classifications of mental pain, along with treatments influenced by industry and centred on pharmaceuticals, has fallen short for many in search of mental health assistance.
The poor mental health outcomes, and the associated social and human costs, compel Whitaker, Wakefield, Moncrieff and Davies to raise systemic questions about the prevailing globally influential mental health care paradigm as found in the United States, United Kingdom, Australia and New Zealand. The consensus among the people interviewed for this series is that there is a pressing need for a thorough examination of the rationalisation and consequences of drug-based treatment choices. At the same time, exploring viable strategies to shield individuals from distress is crucial, and pursuing more effective support mechanisms for those currently experiencing distress is just as essential.
Ultimately, healthcare decisions—including treatment choices—are heavily influenced downstream by political and policy decisions, economic drivers, and ongoing conversations about changing social, religious and cultural expectations. Though often competing, these intermeshed factors guide resource allocation, financial considerations and societal expectations. Notably, mental health, with its inherent ambiguity, is particularly susceptible to economic shifts and changing values, making it even more open to external influences compared to other areas of healthcare.
A non-specialist cannot realistically evaluate the conflicting literature on disorders and psychiatric medications, forcing us to defer to what our health institutions and clinicians tell us—institutions and clinicians working within a limited medicalised set of definitions and institutional pressures. Disturbingly, specialists interviewed for this series underscore a broader issue within the mental health care community. As a collective, professionals and organisations are failing to communicate the uncertainty of research findings and to protect individuals from turning to medication when their emotional struggles fall outside the narrow confines of the claimed evidence base.
Frontline health professionals are not intentionally misleading us. Moncrieff recognises that most health practitioners strive to holistically assess their patients' needs, considering environmental and social stresses, psychological pressures, and biological causes. However, she argues that such comprehensive treatments often differ from what most people receive due to a disconnect between clinicians' intentions and the limitations imposed by institutional structures, such as extremely short consultation times and intermittent follow ups.
They grapple with what Wakefield terms the 'clinician's dilemma’. While all doctors aspire to help alleviate suffering, the dilemma arises when clinicians encounter distressed individuals needing assistance. The primary option within dominant healthcare paradigms is to diagnose and prescribe. Supporting this, United Kingdom doctors report that one in five visits is related to non-medical conditions, such as loneliness or financial problems, for which they are uncomfortable prescribing psychiatric drugs despite having few alternative tools at their disposal.
Moncrieff says that mental health professionals and primary care doctors increasingly tackle the behavioural and emotional consequences of societal issues. These social problems often exceed the capacities of medicine, and the health system can only provide limited assistance to those seeking help. Even if the treatments were effective, "Doctors don't have all the answers!" she emphasises.
Thus, we are also part of the problem. There exist people who grapple with innate, developmental or neurological disorders, which would persist regardless of the societal context. Many people also suffer traumatic reactions to horrific experiences. In such situations, medicine can play a valuable role. Yet, if our distress emerges not from these situations, but more indirectly through prolonged exposure to contemporary society's unhealthy expectations, values and demands, we are uncertain where to seek guidance. In such cases, we encounter neoliberalism’s explanatory framework that prompts us to internalise the issue, assuming the problem lies somewhere within ourselves.
The erosion of traditional social and community support structures under neoliberalism has left healthcare to fill the institutional void. We seek assistance from medicine to address feelings of distress and troubling thoughts, many of which are plausibly ill-served by medicalisation as bonafide disorders. Wakefield suggests that pharmaceutical messaging has normalised the notion that medicine should be the primary recourse for feelings of unease, lack of thriving or troubling thoughts. We also know that opening up about these concerns often leads to a prescription.
However, if as established, a substantial portion of the distress experienced by Anglophiles stems from reactions to the prevalent socioeconomic environment, the limited focus of medicine proves inadequate and potentially harmful.
The medicalisation of mental health issues caused by the environment oversimplifies and harms people by analysing them in isolation from their surroundings. This approach does not help people in distress effectively because it does not address the root cause of the problem. It perpetuates a feedback loop, returning individuals as passive recipients to the same distress-inducing environment. Neoliberal normality significantly exacerbates this issue when it normalises the underlying socioeconomic causes as 'natural’.
Maybe, then, our medical frameworks are simply not the best way to deal with human emotional distress of this sort. Perhaps there are better, more humane ways to support people who haven’t experienced trauma to the point of needing intensive care and monitoring. Alternatives could assist those experiencing milder levels of mental health disorders during periods of unease and crisis.
Individually and systemically, a contextual understanding begins to reveal solutions. Receiving a disturbing diagnosis requires us to be vigilant and not overextend its meaning and impact. Treating it as a general marker of symptoms shared by many others can be valuable. It helps provide coherence to internal suffering that is often hard to understand. Usually, though, a diagnosis is not a life-long determiner of permanent dysfunction or disease. As Whitaker explains, “I’m not the same person I was when I was five, when I was 15, when I was 25 or 35. I’m different from all those people. I don’t experience the world in the same way. If you get depressed at 18, it doesn’t mean you are going to be depressed forever. Human beings are responsive . . . and adaptive to their environments. They are built to change, to be resilient.”
The ways evidence is collated and communicated needs to change. Though this is beyond the scope of what we consider here. Still, the disentanglement of agenda-driven evidence and clinical research is crucial if the evidence for drug treatments is to become more reliable. Critical pressure from policy and patient advocacy bodies such as the United Kingdom’s Council of Evidence-Based Psychiatry, of which Davies and Moncrieff are both members, plays a part. Developing international, centralised, trustworthy and independent trials and reviews for evaluating new medicines is sorely needed. At the very least, our government and regulatory bodies need to provide greater oversight and monitoring of the evidence base. Moves towards transparency in funding and conflicts of interest are essential—but with this must come the enforcement of mandatory disclosure of all study results, whether positive or negative, to avoid selective reporting of favourable evidence.
Positively, a broader shift towards a more dynamic, empowering and less imbalanced care model is gaining traction. The newly released British National Health Service guidelines actively shift away from relying on drug-based care by targeting both antidepressants and heavily sedative pain relief drugs, acknowledging their association with dependence or withdrawal. The guidelines urge all clinicians to limit repeat prescriptions and help wean people off the pills in pursuit of population health outcomes, reduce inequities and promote broader social and economic development.
In a shift that redefines treatment, the guidelines advocate for a collaborative decision-making process between patients and clinicians. This means clinicians must clearly explain both the potential benefits and risks of starting or stopping medications. Moreover, the guidelines prioritise non-drug alternatives, including psychotherapy, social prescribing, health coaching, peer support, talking therapies, and sleep clinics. Notably, clinicians must refrain from prescribing “when evidence-based non-medicine alternatives may be equally or more effective and safer.”
Moncrieff sees such initiatives as positive but thinks a bigger systemic change towards a deinstitutionalised ‘social care model’ needs to occur. Developed in the 1970s, the social care mental health model recognises the interconnected nature of a person's wellbeing, considering cultural influences, economic circumstances, social conditions, and personal characteristics.
From Moncrieff's perspective, the provision of support for individuals grappling with emotional distress or troubling thoughts should predominantly occur outside the confines of a medical framework. This is because the biomedical lens overly emphasises individual bodily deficit and relegates the equally, if not more, significant psychological and social determinants of wellbeing to the sidelines. According to Moncrieff, this oversight hampers a comprehensive understanding of the causes of distress and impedes effective strategies for overcoming it.
The social care model asserts that while biomedical health is a crucial aspect of overall wellbeing, it should not be assigned a central or exclusive role. Instead, mental health is viewed expansively, extending beyond individual factors and emphasising rehabilitation and empowerment through robust social, environmental and economic support systems. The goal is to assist people in forging sustainable paths toward long-term improvement, preventing the recurrence of similar states of distress.
Organisations like the Bromley by Bow Centre in the United Kingdom and Mary's Center in the United States embody transformative social care models that extend beyond a medical care framework. The centres actively strive to enhance an individual's holistic wellbeing, covering physical, psychological, social and economic dimensions. Both integrate the services of medical doctors, psychologists, educators, community mentors and employment advocates to support a person. They facilitate access to education, foster social support networks and inclusion, help find stable housing, and promote employment opportunities.
The centres aim to create a foundation for sustained mental wellbeing by tackling some of the societal factors contributing to mental ill health. In such environments, diagnosis becomes less meaningful and medication less central.
Unsurprisingly, these community centres often serve as articulate voices, readily expressing the repercussions of upstream political and economic decisions. They unveil instances where suffering is a legitimate symptom, highlighting underlying structural issues like economic inequality, wage insecurity and social exclusion.
The social care approach can relieve individuals of the internal burdens of self-blame. By explicitly laying bare the influence of structural forces, community organisations create an awareness that supports personal development and fuels a commitment to advocate for social change. In addition to helping individuals, social care community organisations emerge as formidable advocates for policy changes, standing up against the social and economic forces that fuel widespread distress. Importantly, their advocacy is more transparent, effective and attuned to the nuanced needs of the communities they serve, surpassing the capabilities of traditional medical bodies and public health institutions to push for structural reforms.
Transitioning to community-oriented transformative care models would enable more optimistic, empowering and humane forms of mental health care and support. Uniquely, this model not only tackles symptoms but also focuses on some of the social root causes of mental distress, championing a more active, transparent, extensive and collective approach to our wellbeing.
This series began with the acknowledgement of a seeming paradox. In affluent English-speaking nations, there is a higher prevalence of mental health disorders and the use of psychiatric drugs compared to rates in other countries. Despite relative economic prosperity, abundant material possessions, and widespread access to essential services and human rights protections for most people, individuals in these societies appear more unhappy.
This contradiction prompts questions about what unique factors contribute to widespread distress beyond international averages. The dominance of neoliberal or 'gloves-off' capitalism in many high-income societies, particularly the United States, the United Kingdom, Australia, and New Zealand, is a significant factor. This economic structure, which emphasises individual competition and erodes community and family ties, shapes people's core understandings of themselves. Ubiquitous, it influences all of society to the point we internalise the logic of the gloves-off economic model as natural and commonsensical and the determiner of our success and failure.
The normative distress experienced by large portions of the population in fiercely neoliberal societies suggests that the system itself contributes to stress, uncertainty, disparity and fragility, negatively impacting collective wellbeing. We lose sight of how best to succour and heal ourselves and how crucial relationships with other people and communities are. Seeking help within a healthcare landscape distorted by capitalist opportunism often provides quick-fix treatments for individual deficits. Despite what our mental health institutions tell us—many of us are not mentally sick because of lifelong brain disorders or enduring personal failings. Missing from the biomedical explanatory narrative is a clarification of root causes or advocacy for social change in the interest of collective wellbeing.
Working towards solutions, we need to dismantle the mythic notion that the capitalist abundance of a few equals an abundance for all of us. If we work towards more explicit understanding and change, we must dismantle the separation of clinical practice and advocacy for social justice. As Wakefield notes, "Clinical justice and social justice go hand in hand [in addressing the sources of distress]. I don’t think they can be separated in a benign, caring, humanitarian society."
Many of us in the Anglophile are living through a period of distress, insecurity and unhappiness. We must consider new ways to think of ourselves and find solutions to our shared suffering. At this point in time, the social care model may provide both the space for consolidation and reflection and the catalyst to drive change towards a hopeful and healthy society.



